Invasive
cervical resorption Invasive
cervical resorption
GEOFFREY
S. HEITHERSAY
Invasive cervical resorption (cervical resorption) is
a relatively uncommon form of external root resorption
which has been a source of interest and academic debate
by clinicians and researchers for over a century. Clinical,
radiologic and pathologic features of invasive cervical
resorption provide the basis for a clinical classification
which is of use both in treatment planning and for comparative
clinical research. Although the etiology of this condition
remains obscure, knowledge of potential predisposing
factors is important in assessing patients at risk. Treatment,
where indicated, should aim at the inactivation of all
resorbing tissue and the reconstitution of the resorptive
defect either by the placement of a suitable filing material
or by the use of biological systems.
Invasive cervical resorption is a clinical term used to describe a relatively
uncommon, insidious and often aggressive form of external tooth resorption, which
may occur in any tooth in the permanent dentition (1). Characterized by its cervical
location and invasive nature, this resorptive process leads to progressive and
usually destructive loss of tooth structure. Resorption of coronal dentin and
enamel often creates a clinically obvious pinkish color in the tooth crown as
highly vascular resorptive tissue becomes visible through thin residual enamel.
Essentially, the same resorptive process can occur in other tooth locations:
in erupting teeth it may arise through an enamel defect in the tooth crown and
may be termed invasive coronal resorption, while a more apical source may be
termed invasive
radicular resorption. Invasive cervical resorption has and continues to be misdiagnosed
as a form of internal resorption, a misunderstanding that could possibly be attributed
to the descriptions of internal resorption by Gaskill (2) in 1894 and by Mummery
(3) in 1920 which included teeth showing ‘pink spots’. This pathological process
has obviously intrigued clinicians and researchers for over a century, and still
remains an enigma judging by the current diversity of opinion regarding possible
etiology and pathogenesis. Testiment to this diversity is the nomenclature which
has been applied over the years to this periodontally derived form of external
tooth resorption. The terms include odontoclastoma (4), idiopathic external resorption
(5), fibrous dysplasia of teeth (5), burrowing resorption (6), peripheral cervical
resorption, (7) late cervical resorption (8), cervical external resorption (9),
extra-canal invasive resorption (10), supraosseous extra-canal invasive resorption
(11), peripheral inflammatory root resorption (12), invasive cervical resorption
(1), subepithelial inflammatory root resorption (13, 14), periodontal infection
resorption (15), or simply, and most commonly, cervical resorption (16).
Etiology
Currently, the etiology of invasive cervical resorption is poorly understood
and this may explain some of the diversity in terminology as clinicians have
applied varying interpretations of the underlying pathogenesis. A basic question
to be answered by researchers is whether this resorptive process is purely inflammatory
in nature, activated by sulcular microorganisms, or alternatively a type of benign
proliferative fibrovascular or fibro-osseous disorder in which microorganisms
have no pathogenic role but may become secondary invaders. Current interpretations
rely on an assessment of the clinical manifestations, behavioral characteristics
and the available histopathological material, but a more accurate determination
of the etiology of this disorder will require further molecular biological, enzyme
histochemical or microbiological investigations.
Potential predisposing factors
Several potential predisposing factors have been identified and of these intra-coronal
bleaching has been the most widely documented following the first report by Harrington
and Natkin in 1979 (17) (for a review, see Heithersay et al. (18)).
Trauma,
orthodontics, orthognathic and other dentoalveolar
surgery and periodontal treatment have also been
cited (16, 19). A group of 222 patients with a total
of 257 teeth displaying varying degrees of invasive
cervical resorption have been analyzed by the author
for potential predisposing factors (20) and the results
are summarized diagrammatically in Fig. 1. Figure
1 shows the number of subjects who had either a sole
potential predisposing factor or a combination of
factors. For example of the 33 patients (14.9%) who
had a history of intra-coronal bleaching, 10 (4.5%)
had bleaching as the sole factor, 17 (7.7%) a history
of bleaching and trauma, 2 (0.9%) bleaching and orthodontics
and 4 (1.8 %) a combination of bleaching, trauma
and orthodontics. Of the potential predisposing factors
identified, orthodontics was the most common sole
factor being identified in 47 patients (21.2%) with
62 affected teeth (24.1%), while other factors, principally
trauma and/or bleaching, were present in an additional
11 patients (5%) with 11 affected teeth (4.3%). Trauma
was the second most frequent sole factor with 31
patients (14.0%) with 39 affected teeth (15.1%).
Surgery, particularly involving the cemento-enamel
junction area was identified in 13 patients (5.9%)
as a sole factor. Somewhat surprisingly periodontal
therapy including deep root debridement showed a
low incidence as did other factors such as bruxism.
No potential predisposing factors could be identified
in 33 patients (14.9%).

Fig. 1. Invasive cervical resorption:
Distribution of potential predisposing factors for
patients. From (20). Reproduced with permission from
Quintessence Publishing.
|
|

Fig. 2. Clinical classification
of invasive cervical resorption. From (20). Reproduced
with permission from Quintessence Publishing.
|
Clinical classification
A clinical classification has been developed by the author both for research
purposes and also to provide a clinical guide in the assessment of cases of invasive
cervical resorption (20). The diagrammatic representation of this classification
is shown in Fig. 2.
Class 1 – Denotes a small invasive resorptive lesion near the cervical area with
shallow penetration into dentine.
Class 2 – Denotes a well-defined invasive resorptive lesion that has penetrated
close to the coronal pulp chamber but shows little or no extension into the radicular
dentine.
Class 3 – Denotes a deeper invasion of dentine by resorbing tissue, not only
involving the coronal dentine but also extending into the coronal third of the
root. Class 4 – Denotes a large invasive resorptive process that has extended
beyond the coronal third of the root.

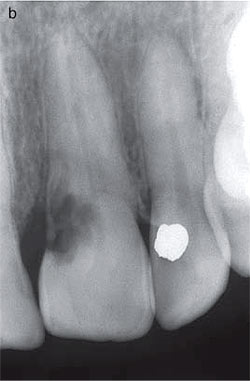
Fig. 3. (a) Labial surface of the dentition of a 19-year-old male.Aslight
reddish irregularity can be seen at the gingival margin of themaxillary
right lateral incisor. (b)Radiograph of the maxillary right lateral incisor.
A small radiolucency
corresponds to the overlying lesion. From (1). Reproduced with permission
from Quintessence Publishing. |
|

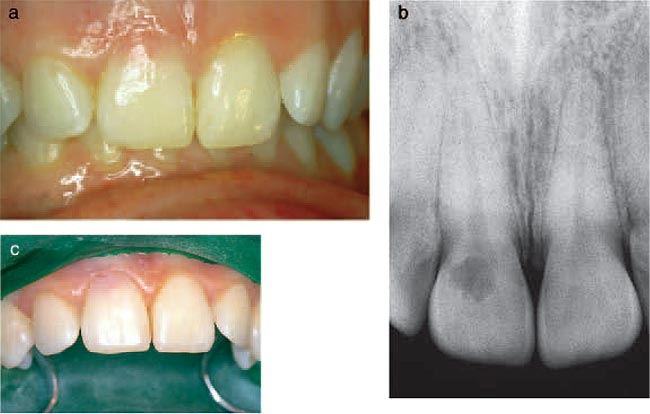
Fig. 4. (a) Labial view of the anterior teeth of a 28-yearold female who
had received fixed orthodontic treatment 14 years earlier. The maxillary
right incisor shows a pink discoloration near the gingivalmargin. (b) The
radiograph of the maxillary right incisor reveals an irregular radiolucency
overlying the root canal outline. From (20). Reproduced with permission
from Quintessence Publishing. |
Clinical, radiologic and
histopathologic features
The clinical presentation of invasive cervical resorption varies considerably
depending on the extent of the resorptive process. The condition is usually painless
and while a pink discoloration of the crown indicates the resorptive process,
some teeth give no visual signs and diagnosis is usually the result of a routine
or sometimes a chance radiologic examination. Multiple resorptionsc an occur,
particularly when there has been a history of orthodontic treatment and a full
mouth radiographic examination should follow the identification of any tooth
showing evidence of invasive cervical resorption. The study of potential predisposing
factors showed that the majority of patients presented at a Class 3 stage of
resorption, which is indicative of the diagnostic difficulties encountered with
this resorptive process (20). The following will outline the clinical, radiographic
and histopathologic features of the four Classes of invasive cervical resorption
as defined above.
Class 1
Some early lesions which are in this category may show a slight irregularity
in the gingival contour associated with a surface defect containing soft tissue
which bleeds on probing (Fig. 3a). A radiograph will usually show a small coronal
radiolucency corresponding to the lesion (Fig. 3b).
Class 2
Invasive resorptive lesions of this class may present with a pink discoloration
of the tooth crown (Fig. 4a), while the radiographic image usually shows a surprisingly
extensive irregular radiolucency extending from the cervical area into the tooth
crown and projected over the root canal outline (Fig. 4b). If the lesion is proximally
located the radiographic image will show ar adiopaque line bordering the pulp
space. An examplec an be seen in a radiograph of the maxillary central
incisors of a 22-year-old male who had a history of extensive orthodontic treatment
in his teens (Fig. 5a).W hile this image is similar to that of dental caries,
it
differs in that the outline is slightly more irregular. The clinical appearance
of the palatal surface of this patient postulated that pulpitic symptoms only
develop when the resorption ultimately penetrates through this barriera nd is
secondarily invaded by oral microorganisms.E vidence for the presence of an anti-invasion
factor in predentin has been presented (21) and provides ane xplanation for this
uniquely interesting protectiveb arrier observed in this active formof tooth
resorption.


Fig. 5. (a) Radiograph of the maxillary central incisors of a 22-year-old
male. Extensive radiolucent areas extend close to the pulp spaces. Although
similar in appearance to carious lesions, the margins are somewhat irregular.
The pulp space is bordered by a radiopaque line which is more evident in
the right incisor. The invasive cervical resorptive lesion is classified
Class 2. (b) Palatal surfaces of the maxillary central incisors. Pinkish
area are visible near the mesial cervical regions, particularly evident
in the right incisor. From (1). Reproduced with permission from Quintessence
Publishing.
|
|


Fig. 6. (a) Radiograph of a mandibular left molar of a 17- year-old male.
An irregular mottled radiolucency extends from the distal margin into the
crown and adjacent to the pulp space but is separated by a radiopaque line.
The
invasive cervical resorptive lesion is classified as Class 2. (b) Crown
of the mandibular left molar showing no external signs of resorption. From
(1). Reproduced with permission from Quintessence Publishing. |
Class 3
In this category the invasive resorptive process hasr adicular extensions into,
but not beyond, the coronal third of the root. Clinically, the crown of an involved
tooth may show a pink discoloration, and there may bec avitation of the overlying
enamel. Figures 8a and 9ashow degrees of enamel cavitation in two Class 3 cases,
the first a 24-year-old-male whose maxillary anterior teeth had been hit by a
cricket ball approximately 9 years earlier and the second, a 19-year-old male
who had received orthodontic treatment at age 12. In these examples, the teeth
were asymptomatic and it was only the changed appearance in the first case and
an altered oral perception in the second that prompted dental examinations. Symptoms
rarely occur in Class 3 casesu nless there has been superimposed infection in
the
pulp or periodontium.

Fig. 7. Histologic appearance of an incisor tooth with invasive resorption.
An intact layer of dentine and predentine on the pulpal aspect (n)
separates the pulp from the resorbing tissue. The resorption cavity
is filled with a mass of fibrovascular tissue with active mononucleated
and multinucleated classic cells lining resportion lacunae (arrows).
(Hematoxylin–eosin stain; original magnification 40.). (Courtesy of
Dr John McNamara.) From (1). Reproduced
with permission from Quintessence Publishing.
|
|


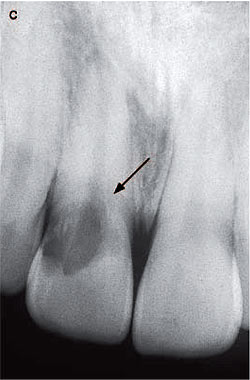
Fig. 8. (a) The maxillary right central incisor of a 24- year-old male
shows a pinkish discoloration and slight cavitation near the disto-gingival
margin. (b) Radiographic appearance of the maxillary right central incisor
reveals an irregular ‘moth-eaten’ radiolucency on the distal aspect of
the tooth extending to the outline of the root canal and into the root
(arrow). The invasive cervical resorptive lesion is classified as Class
3.
|
The radiographic appearance generally shows ani rregular mottled, or ‘moth-eaten’
image in the main lesion area and the outline of the root canal can be seenas
a radiopaque line demarcating the root canal from the adjacent irregular radiolucency,
the latter being indicative of resorbing tissue. Figures 8b and 9c illustrate
these radiographic features. In most instances in the study of 222 patients with
257 affected teeth referred to above, the radiographic appearance of the crestal
bone remained unchanged except in a few instances were there was clinical evidence
of superimposed infection of the adjacent periodontium. An example of a localized
gingival infection associated with invasive cervical resorption can be seen in
Fig. 10a, which shows the clinical appearance of a maxillary left central incisor
of a 35-year-old female. A radiograph of the tooth shows radiolucencies in both
the tooth and
the crestal bone (Fig. 10b).
The histopathologic appearance of a tooth displaying radicular extension of invasive
root resorption is shown
in Figs 11a, b.
 |
|
 |
Fig. 11. (a) Histologic appearance of an extensive invasive cervical resorption
with radicular extensions. Masses ofe ctopic calcific tissue are evident both
within the fibrovascular tissue occupying the resorption cavity and on resorbed
dentin surfaces. In addition, communicating channels can be seen connecting with
the periodontal ligament (large arrows). Other channels can be seen within the
inferior aspect of the radicular dentine (small arrows). (Hematoxylin–eosin stain;
original magnification 30.) (b) Higher magnification of (a) showing communication
channels from the periodontal ligament to the resorbing tissue. An island of
hard tissue remains (n), consisting of an external surface of cementum and cementoid,
some residual dentine but the bulk has been replaced with a bone-like material
with canalicular structure. Although some red blood cells are evident near the
deeper channel no inflammatory cells can be seen. (Hematoxylin-eosin stain; original
magnification 50.) From (1). Reproduced with permission from
Quintessence Publishing.
The radicular tooth structure shows an extensive resorptive defect containing
a mass of fibroosseous tissue, while at the base of the defect, bone-like tissue
has been deposited on resorbed dentin. In addition, there are infiltrating channels
containing soft tissue with communications with the periodontal ligament. The
entire region is devoid of inflammatoryc ells, which is consistent with another
specimen published by the author (22) and some previous observations (4–7). A
cross-sectional view of a tooth with invasive cervical resorption is shown in
Fig. 12. The intact pulp is surrounded by a complex network of fibro-osseous
tissue which has replaced normal tooth structure. No inflammatory cells can be
seen either in the pulp or within the resorption tissue. The walling off of the
pulp space in this type of resorption is further illustrated in Fig. 13, which
shows a high magnification cross-sectional photograph of a tooth which has been
subjected to extensive invasive cervical resorption. There have been similar
histopathologic observations in respect to the presence of irregular calcified
deposits within the resorbed areas of teeth displaying invasive cervical resorption,
but the presence of minimal to moderate inflammatory cellular infiltrates in
some regions have been noted (7, 9, 19). This occurred in one of the two cases
reported by Southan (7). A similar infiltration of inflammatory cells into the
resorptive tissue is shown in Fig. 14 taken from a tooth with a large invasive
cervical resorptive lesion and an associated periodontitis. Some authors consider
the resorptive tissue to be identical with other forms of progressive inflammatory
root resorption, which are characterized by the presence of inflammatory cells,
multinucleated clast cells, granulation tissue and resorption lacunae in both
tooth and bone (13, 14).

Fig. 12. Histologic appearance of a cross sectional view of an incisor
tooth showing an intact pulp encircled by a narrow band of dentin and surrounded
by an extensive resorptive lesion containing fibro-osseous tissue. (Hematoxylin
and eosin stain. Original magnification x 10).

Fig. 13. A low-powered photograph shows the walling off of the pulp space
by dentin separating it from the surrounding extensive resorptive process.
|
|

Fig. 14. Mass of fibrovascular tissue infiltrated with inflammatory cells,
located within a large resorptive cavity that has a wide connection with
the periodontal
tissue (large arrow). The dentin has been extensively replaced by bone-like
tissue. A small section of intact pulp can be seen on the superior aspect
of the section (small arrow). Hematoxylin–eosin stain; original magnification
x 30.) From (1). Reproduced with permission from Quintessence Publishing. |
Class 4
This category includes invasive resorptive processest hat have extended beyond
the coronal third of the rootand an example is shown in Figs 15a, b: a maxillary
left central incisor of a 28-year-old male who had a history of dental trauma
some years earlier. While the crown displayed a pink discoloration in the cervical
region, the radiograph shows, in addition to the irregular outline of the resorptive
process in the tooth crown, radiolucent lines extending alongside the pulp space
into the apical third of the root. In a further example of a Class 4 resorption,
overt signs and symptoms of ana cute periodontal infection (Figs 16a, b) gave
the first indication to the 38-year-old female patient of the extensive resorptive
process that had developed in her maxillary left central incisor.One histopathologic
specimen of a Class 4 invasive cervical resorption is shown in Figs 17a, b a
crosssectional view of a maxillary incisor showing extensive replacement of tooth
structure including the dental pulp by bone-like calcified tissue, and spaces
containing fibrovascular tissue. No inflammatory cells could be observed in this
specimen, but they would be expected
if infection were to supervene.


Fig. 15. (a) An extensive pink area can be seen in the cervical region
of the maxillary left central incisor of a 28-year-old male. The adjacent
soft tissues appear normal. (b) The radiograph of the maxillary left central
incisor reveals a large coronal radiolucency and irregular radiolucent
lines extending deeply into the root (arrows). The outline of the pulp
space can be identified by radiopaque lines. This invasive cervical resorptive
lesion is classified as Class 4. From (23). Reproduced with permission
from Quintessence Publishing. |
|


Fig.16. (a) Maxillary left central incisor of a 38-year-old female. Infection
involving the tooth and the periodontium is evidenced by local inflammation
with
exudation at the gingival margin. (b) Radiograph of the maxillary left
central incisor. An extensive but diffuse, irregular radiolucency extends
to the crownand deeply into the root (arrows). Areas of increased radiolucency
appear near the cervical region, corresponding to the location of the periodontal
infection. From (1). Reproduced with permission from Quintessence Publishing. |
 |
|
 |
Fig. 17. (a) Cross-sectional view of an incisor tooth,showing complete replacement
of the pulp space andsurrounding dentin by bone-like tissue with spacescontaining
fibrovascular tissue. At the periphery, somecementum has also been resorbed (arrow).
A residual scalloped band of dentin (D) and cementum remains elsewhere. (Hematoxylin–eosin
stain; original magnification 10.) (b) Higher magnification of (a) showing thebone-like
structure of the central radicular section. No recognizable pulp space is present,
but there are irregular spaces containing fibrovascular tissue. Note the presence
of many small concentrically located channels. (Hematoxylin– eosin stain; original
magnification x 50.) From (1).
Reproduced with permission from Quintessence Publishing.
Clinical management
The clinical classification outlined above was developed both as a research tool
and a practical guide to allow comparative assessments of the results of various
nonsurgicalor surgical treatment regimens. Clearly as thepathological manifestations
of the various classes ofinvasive cervical resorption become more complex,
differing non-surgical or surgical treatment will be required. Nevertheless the
basic aim remains the same, namely the inactivation of all active resorbing tissue
and
the reconstitution of the resorptive defect either by the placement of a suitable
filling material or by the use of biological systems such as membranes, so that
the tooth may be healthily and aesthetically retained. Non-surgical treatment
As a basis for discussion, a treatment regimen proposedby the author will be
outlined along with the results of such treatment applied to 101 teeth from 94
patients displaying varying degrees of invasive resorption and followed up for
a minimum of 3 years (23). The nonsurgical treatment involved the topical application
of a 90% aqueous solution of trichloracetic acid to the resorptive tissue, curettage,
endodontic treatment where necessary, and restoration with glass-ionomer cement.
Adjunctive orthodontic extrusion was also employed in some advanced lesions.
The following case reports illustrate this treatment regimen applied to a Class
2 and a Class 3 category invasive cervical resorption. Illustrative Class 2 treatment
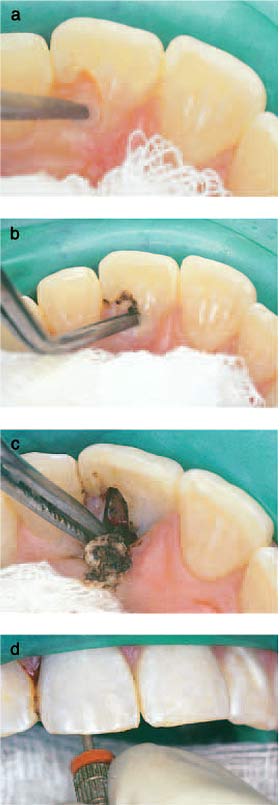
A 21-year-old female, with a history of dental trauma showed an invasive cervical
defect in the coronal aspect of her maxillary right central incisor which on
clinicaland radiographic grounds was classified as Class 2 (Figs 18a, b). After
protective application of glycerol toadjacent soft tissues and the placement
of a glycerolimpregnated cotton roll into the labial sulcus, rubber dam was applied
using a cuff technique (Fig. 18c). A small cotton pellet (size 000 divided in
half) which had been dipped into a very small quantity of a 90% aqueous solution
of trichloracetic acid and then dampened on gauze, was applied for 1-2 min with
gentle pressure to the resorptive lesion which was accessible through an enamel
defect near the gingival margin (Fig. 18d). The pressure was slowly increased
as the medicament caused progressive coagulation necrosis of the resorptive tissue
and there was a collapse of the thin overlying enamel (Fig. 18e). The devitalized
avascular tissue was curetted from the resorption cavity, which was then carefully
checked under magnification with an enhanced light source. This examination revealed
an intact smooth dentine floor cavity with no communication with the dental pulp
(Fig. 18f). The cavity margins were then smoothed with a high-speed tungsten
carbide bur under water spray and the defect restored with a glassionomer cement,
protected with a light-activated unfilled bonding resin (Fig. 18g). Follow-up
examinations to 5 years did not reveal any evidence of pulpal or periapical pathology
or continuation of the resorptive process, and the restoration and adjacent gingival
tissues were assessed as most satisfactory (Figs 18h, i). If there had been obvious
pulp involvement on removal of the resorptive tissue, pulpectomy would have been
carried out accessing the canal via the resorption cavity to retain as much residual
tooth structure as possible. A similar treatment regimen to the illustrative
Class 2 case shown above can be applied to a Class1 category of invasive cervical
resorption.
Fig. 18. (a) The maxillary right central incisor of a 21- year-old woman shows
a pink discoloration on the labial aspect of the crown. The tooth had been traumatized
9 years earlier. (b) A radiograph of the maxillary right central incisor reveals
an irregular radiolucency overlying the root canal with no obvious extensions
into the root canal. This invasive cervical resorptive lesion is classified as
Class 2. (c) After a protective application of glycerol to adjacent soft tissue,
a rubber dam ‘cuff’ has been placed for protection and isolation. This has been
supplemented with a glycerol-impregnated cotton roll placed in the labial sulcus.
(d) Trichloracetic acid on a small cotton pellet is applied to the resorptive
defect with slowly increasing pressure, so that the resorptive tissue within
the cavity undergoes coagulation necrosis. (e) The appearance of the tissue within
the resorptive defect following the application of trichloracetic acid indicates
tissue necrosis. The adjacent whitened gingival tissues indicate a limited zone
of coagulation necrosis. (f) Following curettage of the avascular tissue from
the resorption cavity, the glistening dentinal base of the cavity is revealed.
The incisal margin of the cavity has been smoothed with high-speed bur under
water spray. (g) A glass-ionomer restoration has been placed in the cavity, and
its surface has been protected with a light-activated unfilled bonded resin.
(h) Clinical appearance of the tooth 5 years postoperatively. The original glass-ionomer
cement has been faced with a resin composite restoration. (i) A 5-year follow-up
radiograph of the maxillary right central incisor shows no evidence of periapical
pathosis or extension of the treated resorptive lesion. From (23). Reproduced
with permission from
Quintessence Publishing.
Illustrative Class 3 treatment
The maxillary right central incisor of the 19-year-old male shown earlier in
Figs 9a, b&cwas treated following the preparation and protection procedures
outlined for the illustrative Class 2 case. Trichloracetic acid was applied on
a small cotton pellet to the resorptive tissue on the palatal aspect of the tooth
for approximately 3 or 4 min (Fig. 19a): the medicament was replenished on at
least two occasions, and the pressure on the cotton pellet was slowly increased
as the tissue within the resorption cavity became progressively avascular due
to a process of coagulation necrosis (Fig. 19b). In this way, the majority of
the coronal component of the resorption cavity could be accessed and then simply
removed by curettage (Fig. 19c). Although an apparently sound base was present,
elective pulpectomy was carried out to allow access to the more deeply infiltrating
tissue encircling the root canal (Fig. 19d). The canal was prepared with hand
instruments and then enlarged with Gates–Glidden drills particularly in the coronal
third of the root canal to engage the encircling resorptive tissue. Further application
of trichloracetic
acid and curettage allowed complete visualization of the resorption defect with
the aid of 5.5 magnification and a focussed helium light source (Fig. 19e). The
canal was then dressed with a corticosteroid, antibiotic paste (Ledermix paste;
Lederle Pharmaceuticals, Wolfratshausen, Germany), a therapeutic combination
which has been shown to exhibit anti-clastic activity (24–26), and the defect
was temporarily restored with Cavit (3m ESPE, Seefeld, Germany). At a subsequent
appointment,18 days later, the temporary filling and intracanal dressing material
were removed by irrigation and sonication. After the canal had been dried, careful
inspection with enhanced vision did not reveal any sign of further vascular channels,
the resorption cavity was well defined and the adjacent soft tissues showed satisfactory
healing (Fig. 19f). The canal was then
obturated with gutta-percha and AH26 (Dentsply/
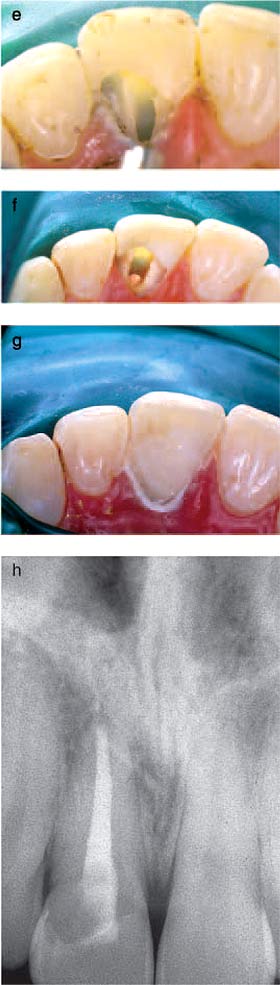
Fig. 19. (a) The topical application of trichloracetic acid on a small cotton
pellet is carried out with slowly increasingpressure to prevent haemorrhage.
(b) Continued application of trichloracetic acid on a small cotton pellet with
pressure allows the deeper regions of the lesion to be rendered avascular by
the process of coagulation necrosis. (c)The affected tissue is curetted from
the resorptive cavity to reveal the apparent dentinal base. (d) Elective pulpectomy
is carried out in
the central incisor, to allow access to encircling resorptive tissue. (e) Following
pulpal extirpation, the canal has been enlarged in the coronal third with Gates–Glidden
drills to exclude any resorptive tissue surrounding the root canal. Topical application
of trichloracetic acid has allowed tissue destruction in the resorptive cavity,
which has then been thoroughly curetted. (f) The root canal has been sealed with
gutta-percha and
AH26 18 days after pulpectomy, intracanal
dressing with Ledermix paste, and coronal sealing with Cavit. The gingival tissue
show good healing and the margins of the resorption cavity are well defined.
(g) A glass-ionomer restoration has been inserted into the resorption cavity
following a further topical application of trichloracetic acid to aid in moisture
control. (h) The postoperative radiograph of the maxillary right central incisor
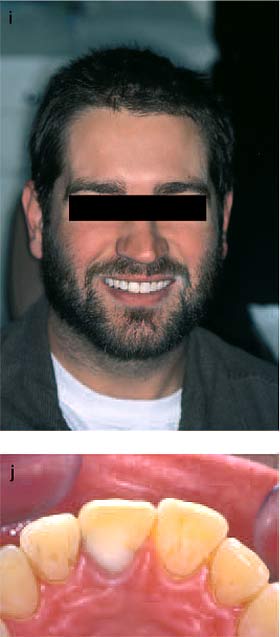
indicates satisfactory filling of the resorptive defect. (i) The labial appearance
10 years after treatment shows a satisfactory aesthetic result. (j) After 10
years, the palatal gingival tissues appear healthy. The original glass-ionomer
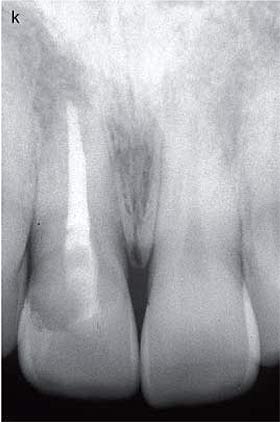
restoration has been refaced because of some surface creasing. (k) A 10-year
follow-up radiograph shows no evidence of further resorption or periradicular
pathology. From (23). Reproduced with
permission from Quintessence Publishing.
DeTrey, Konstanz, Germany). A further brief application of trichloracetic acid
ensured a dry field for the
insertion of a glass-ionomer cement restoration which
was protected with a light-activated unfilled bonding resin (Fig. 19g). The patient
has been re-examined at
regular intervals and the clinical and radiographic
appearance of the tooth 10 years after treatment are shown in Figs 19h–j. Orthodontic
extrusion can be used to advantage in some Class 3 resorptions by improving access
to the base of the resorption cavity and providing a supragingival margin for
the restoration (27–30). Extrusion is usually effected over 4–6 weeks, using
a light wire technique, and this is followed by splinting, pericision, gingivoplasty
and finally restoration. An internal approach is possible in some Class 3 resorptions
but it is essential that the resorptive tissue be traced to the external point
(or points) of entry and inactivated by the topical application of trichloracetic
acid prior to the internal placement of a glass-ionomer cement. Alternatively,
the defect could be filled with the mineral trioxide aggregrate material, Pro-Root
MTA (Dentsply Tulsa Dental, Johnson City, TN, USA), which would appear to possess
ideal properties for this
type of repair (31, 32).
The results of the study of the treatment of 94 patients with 101 teeth affected
by various degrees (Classes 1–4) of invasive cervical resorption showed complete
success in Class 1 and Class 2 resorptions, judged by an absence of resorption
and periradicular or periapical pathology. The follow-up periods for the Class
1 cases varied from 3 to 8 years (mean 4.5 years) and Class 2 cases varied from
3 to 12 years (mean 8 years). Of the 63 teeth classified with Class 3 invasive
cervical resorption, 61 (96.8%) showed resorption control. Five teeth (7.9%)
had been extracted during the review period, which varied from 3 to 12 years
(mean 5.5 years), 1 (1.6%) because of continuing root resorption, 3 (4.7%) because
of root fracture and 1
(1.6%) because of previous traumatic bone loss. The
mean survival time of the teeth which had been extracted was 5.8 years. The gingival
response was
clinically satisfactory in 59 teeth (93.7%), but there was
evidence of some angular bone loss in 4 teeth (6.3%) and small periapical radiolucencies
were observed in 5
teeth (7.9%). When all factors (resorption control,
angular bone loss, periapical changes and extraction) were included in the assessment,
the overall success rate of Class 3 treatments was 77.8%. Endodontic retreatment
of the five cases with evidence of periapical pathology and orthodontic extrusion
and periodontal management of the four cases with angular bone loss may have
enhanced this success rate.
In Class 4 resorptions 16 teeth were treated and the results showed a survival
rate of 50.0% and a success rate as judged above 12.5%. This represents anunsatisfactory
outcome for this treatment regimen when applied to Class 4 resorptions, and alternative
prosthodontic replacement is generally suggested. However, there are occasions
when treatment may be justified, provided it does not compromise supporting bone.
Orthodontic extrusion is invariably required as
an adjunctive treatment if a successful result is to be achieved. Another option
in some cases of Class 4 invasive cervical resorption is to leave the affected
tooth
untreated; however, this may put at risk the health of the supporting bone as
a site for implant placement should superimposed periodontal infection develop.The
rate of resorption in Class 4 cases has not been investigated but clinical observations
suggest that in the absence of superimposed infection, the progress in older
patients is slow.
A non-surgical approach for some resorptions hasbeen suggested by Frank (33)
who pioneered many of the early clinical studies of this type of resorption.
When
the resorption was intra-osseous, Frank emphasized the importance of the removal
of all resorptive tissue to what he termed the portal of entry. This was carried
out with a large round bur and the cavity was then filled
with amalgam.
Surgical management
Surgical treatment of varying degrees of invasive cervical resorption has generally
involved periodontal
flap reflection, curettage, restoration of the defect with
amalgam (10, 11, 16, 34), composite resin (8, 35) or glass-ionomer cement (8,
22) and repositioning the
flap to its original position. Periodontal reattachment
cannot be expected with amalgam or composite resin, and is unlikely with glass-ionomer
cement, but there is
experimental evidence to suggest that this might be
possible should MTA be used in this situation (31, 32). An alternative surgical
option is to apically position the flap to the base of the resorption repair:
However,
should this prove aesthetically unacceptable, orthodontic extrusion can be utilized
to improve the gingival contour (36). Rankow has developed innovative treatment
methods that utilize a Gortex membrane (W.L. Gore Inc., Elkton, MD, USA) for
guided tissue regeneration in various forms of endodontic surgery, including
(invasive) cervical resorption (37). In one such case in which the gingival attachment
was intact, flap reflection allowed the resorptive lesion to be accessed from
the buccal aspect. Following curettage, pulpectomy and root filling of the canal
apical to the resorptive defect and composite filling of the coronal access cavity
to the level of the defect, a Gortex membrane was placed without any restoration
of the resorption cavity. The Gortex membrane was removed after 6 weeks. A follow-up
radiograph taken 4 years after this treatment showed evidence of resorption control
and no sign of periradicular pathology. Other surgical treatment strategies have
recently been outlined including other resorption cases treated using a guided
tissue regeneration
technique (38).
Discussion Invasive cervical resorption is a relatively uncommon and clinically
challenging condition with an academically debatable pathogenesis. The invasive
and somewhat aggressive characteristics of the process, coupled with its histopathologic
features, raise questions as to the nature of the lesion. The invading tissue
arises from the periodontal ligament but differs from periodontal tissues in
both structure and behavior. The precursor cells of the periodontal ligament,
being ectomesenchymal in origin, have the potential to differentiate into cells
capable of laying down fibrous tissue or calcified tissue (39). For invasion
to occur, a defect in the cementum/cementoid layer is a likely prerequisite (7,
40, 41). This may be of developmental origin in a small zone near the cervical
area, or the result of physical or chemical trauma. Such a cementum–cementoid
deficiency allows direct contact between dentin and the potentially resorptive
cells of the periodontium.
What then causes the activation of resorption and the invasion of this fibrovascular/fibro-osseous
tissue? There is one body of opinion that considers sulcular microorganisms to
be the activating factors (12, 13, 15, 16, 19). A hypothesis has been advanced
to support this etiology and to explain the delayed nature of this process which
occurs in some patients. The hypothesis suggests that an inflammatory process
in the periodontium at the attachment level does not reach a damaged root surface
initially, and that it is only with eruption of the tooth or gingival recession
that inflammatory mediators can attract resorbing cells to the root surface (19).
Some of the limited published histopathologic material showing inflammatory cellular
infiltrates may provide support for this opinion and
hypothesis (7, 9, 19).
Nevertheless, there are contrary arguments. The presence of inflammatory cells
is not necessarily indicative of a microbiological etiology and there are cases
in the literature, which show no inflammation (1, 5, 7, 42). These cases, coupled
with the clinical manifestations, indicate that invasive cervical resorption
is an aseptic resorptive process, which may on occasions become secondarily invaded
with microorganisms.
The reason for an apparent varying lag phase of months to years between a particular
insult to the root
surface at or near the cemento-enamel junction and the
development of invasive cervical resorption remains conjectural. A simple clinical
explanation may be that
early lesions are not being detected because of inherent
difficulties in diagnosis, and their detection at a later stage gives a false
impression of a lag time. This was evident in the clinical study of 222 patients
where only
six patients were diagnosed at a Class 1 stage, while the majority were detected
at the relatively advanced Class 3 stage. (20) In addition, the clinical study
did not show significant clinical evidence of gingival recession, marginal gingivitis
or periodontitis in the majority of patients presenting with various degrees
of invasive
cervical resorption, contrary to the periodontal infective hypothesis advanced
above. Nevertheless, the hypothesis does provide a logical explanation for secondary
or superimposed infection of an established lesion as illustrated in the two
cases shown in Figs 10a,
b and 16a, b. Operative procedures have also been
reported as a potential cause of secondary bacterial invasion of these lesions
(1).
There may be a non-bacterial explanation for this resorptive process involving
a breakdown in an antiresorptive biologic control mechanism originating in the
periodontal ligament and possibly exerted by epithelial cells of the rests of
Malassez (43–45). Recent research into clastic cell activity in a model of aseptic
root resorption provides additional support for the progression of resorption
in the absence of periodontal
epithelial rests (46).
It appears that all types of dental resorption share common cellular mechanisms.
Resorption of teeth results from the activation of clastic cells, termed odontoclasts,
which are morphologically similar, if not identical, to osteoclasts. The structure
and function of osteoclasts has been extensively studied and reviewed (47–49).
Certain features of dental resorption appear to be common to all the different
types. Over recent years, there have been significant advances in the understanding
of osteoclast differentiation and activation due to the analysis of a number
of factors involved in a RANK (receptor activator of nuclear factor k B) signalling
network in osteoclasts. The factors which have been analyzed include a family
of biologically related tumor necrosis factor (TNF), tumor necrosis factor receptor
(TNFR)/TNF-like proteins: osteoprotegerin (OPG), RANK and RANK ligand (RANKL)
which collectively regulate osteoclast function (49). This system may be activated
following physical, chemical or microbiological insults or by a post-zygotic
gene (50).
Classical external inflammatory (infective) root resorption has been studied
extensively and usually follows tooth luxation or avulsion where there has been
cemental damage and pulp necrosis with bacterial invasion (51). The osteolytic
inflammatory response to the bacterial products, which pass from the pulp space
to
the external surface of the root involves the activation of clast cells resulting
in resorption of both tooth and bone. This type of resorption is radiographically
recognizable as bowl-like radiolucencies in both the involved tooth and the adjacent
bone. An example can be seen in Fig. 20 that shows a maxillary central incisor,
which had been avulsed and replanted 6 months earlier. The histopathological
appearance of a tooth exhibiting external inflammatory root resorption is shown
in Fig. 21. Observable features include the presence of multinucleated clast
cells at the dentin and bone interface, chronic inflammatory cellular infiltrates,
and the
scalloped appearance of the resorbed dentin and bone.

Fig. 20. Radiograph showing evidence of extensive
external inflammatory root resorption in a 9-year-old female whose avulsed
maxillary left central incisor had been replanted 6 months earlier. She
had unfortunately failed to attend follow-up examinations. |
|

Fig. 21. Histologic appearance of a tooth exhibiting
external inflammatory root resorption, showing multinucleated clast cells
adjacent to resorbed dentin and bone. A chronic inflammatory cellular infiltrate
is also evident in the area. (Hematoxylin and eosin stain. Original magnification
x 50.) (courtesy Dr Angela Pierce.) |
There appear to be differences in the behavior, pathology and radiographic features
of many cases of invasive cervical resorption to that of the classically described
external inflammatory root resorption. In invasive cervical resorption, the pulp
survives until late in the resorptive process, being protected by a layer of
predentin and dentin, while the pulp is necrotic and infected before external
inflammatory root resorption
occurs. The progressive resorption in invasive cervical
resorption is characterized by the ingrowth of fibrovascular tissue in the early
stages and later by fibroosseous tissue, which is also laid down on the resorbed
surface of dentin. Resorption channels are created which burrow into dentin and
may interconnect with the periodontal ligament. While areas of both resorption
and hard tissue repair can be observed in some cases of external inflammatory
resorption, the other fibro-osseous responses seen in invasive cervical resorption
appear to be unique to this external, periodontally
derived tooth resorption.
Invasive cervical resorption was classically described byWade in 1960 as one
in which there were alternating periods of resorption and repair with ultimately
the former outstripping the latter (5). This author also suggested that the process
was similar to that found in fibrous dysplasia of bone and, as such, could be
regarded as fibrous dysplasia of the tooth. There are indeed similarities between
the histopathologic appearance of invasive cervical resorption and that of fibrous
dysplasia of bone, giving support to this early concept. Fibrous dysplasia of
bone is gene related and classified by the World Health Organisation as a tumor-like
lesion (52). In view of the histopathology and behavioral characteristics of
invasive cervical resorption, it is suggested that the condition could be labelled
as a progressive
fibrous or fibro-osseous disorder of teeth.
The radiographic interpretation of invasive cervical resorption is critical to
diagnosis and treatment. It is important to differentially diagnose this externally
derived resorption from that of internal root canal inflammatory resorption and
internal root canal replacement resorption as defined by Andreasen and Andreasen
(53). Internal root canal inflammatory resorption can be identified as a uniform
enlargement of the root canal. Internal replacement resorption is more difficult
to diagnose from external invasive cervical or radicular resorption because the
resorptive tissue has the same histopathologic characteristics and accordingly,
has a similar radiographic appearance. Although the lesion has been classified
as a form of internal root canal resorption, there has been experimental evidence
to suggest the resorbing tissue is also derived from the periodontal ligament
(54). In the case of internal replacement resorption, there is an absence of
the radiopaque line of demarcation between the root canal and the image of resorption
in dentin.
Invasive cervical resorption has often been diagnosed in the past as internal
resorption. In 1971 the suggested pathogenesis of some ‘internal’ resorptive
lesions,
which clearly had external connections, was an extension of a pulpally derived
internal resorption to involve the periodontal ligament (55). Later, a landmark
study
carried out by Makkes and Thoden Van Veltzen (9) demonstrated an external periodontal
source for
(invasive) cervical root resorption.
While the exact nature of this interestingly complex pathological process remains
debatable, the treatment
of invasive cervical resorption poses particular clinical
problems. The aggressive nature of this type of resorption varies, and despite
apparent complete removal of the resorptive tissue, in some cases it may recur.
This may be due to the development of new resorption adjacent to or remote from
the original site.
Alternatively, there may be a concurrence or continuation
of the resorption due to incomplete inactivation of resorptive tissue particularly
in the deeply penetrating
channels which are a feature of this type of resorption.
The rationale for the topical application of trichloracetic acid in the treatment
of these resorptive lesions was to utilize the proven action of this chemical
agent in
inducing coagulation necrosis while adjacent tissues remain free of inflammation
(42). It was anticipated that this chemical agent would affect not only the resorptive
tissue in the body of the lesion, but also the tissue contained in the deeper
and often interconnecting channels. The results of the clinical study in which
trichloracetic acid was used as an agent in the treatment of various degrees
of invasive cervical resorption (23) can at least provide a basis for comparison
with other treatment modalities, which to date have only been detailed in a series
of case reports with follow-up periods varying from a few months to a maximum
of 10 years (56).
Guided tissue regenerative techniques are attractive treatment alternatives but
further clinical research is desirable to assess the overall success of these
and other regenerative methods. Another possible avenue of treatment involves
the application of a combination of Emdogain (Biora, AB Malmo, Sweden) and Bio-oss
(Osteohealth, Luitpold Pharmaceuticals, Shirley, NY, USA), which has been used
to apparent advantage in regeneration of some localized periodontal lesions with
bone loss (57, 58). The technique has the advantage that a membrane is not required.
The topical application of bisphosphonates, anticlastic agents used in the treatment
of osteoporosis, may offer another possible therapy. Fortunately, invasive cervical
resorption is a relatively uncommon condition but for patients affected by this
pathological process, it can cause great concern. Identification of potential
predisposing factors may allow some preventive measures to be implemented, but
hopefully further research into the etiology and pathogenesis of this resorptive
process will provide the basis for improved methods of treatment. Invasive cervical
resorption also occurs in cats, and as similar clinical, radiologic and histopathologic
features have been reported (59, 60), there may be the possibility for other
avenues of research into this challenging pathological condition.
Acknowledgements
The author wishes to acknowledge Quintessence International for their permission
to reproduce figures from his original publications in that Journal. In addition
he wishes to thank Helen Heithersay, Dr Angela Pierce, and Dr Fabrizio Damiani
for their valued help in the preparation of this paper.
References
1. Heithersay GS. Clinical, radiologic, and histopathologic features of invasive
cervical resorption. Quintessence 1999: 30: 27–37.
2. Gaskill JH. Report of a case of internal resorption. Dental Cosmos 1894: 36:
1019–1024.
3. Mummery JH. The pathology of ‘pink spots’ on teeth. Br Dent J 1920: 41: 301–311.
4. Fish EW. Begnign neoplasia of tooth and bone. Proc R Soc Med 1941: 34: 427–432.
5. Wade AB. Basic Periodontology. Bristol, England: Wright @ Sons, 1960: 156–159.
6. Seward GR. Periodontal diseases and resorption of teeth. Br Dent J 1963: 114:
443–449.
7. Southan JC. Clinical and histological aspects of peripheral cervical resorption.
J Periodontol 1967: 38: 534–538.
8. Cvek M. Endodontic treatment of traumatised teeth. In Andreasen JO, ed. Traumatic
Injuries to the Teeth, 2nd edn. Copenhagen: Munksgaard, 1981: 362–363.
9. Makkes PC, Thoden Van Veltzen SR. Cervical external root resorption. J Dent
1975: 3: 217–222.
10. Frank AL. External–internal progressive resorption and its non-surgical correction.
J Endod 1981: 7: 473–476.
11. Frank AL, Blakland LK. Supra osseous extra-canal invasive resorption. J Endod
1987: 13: 348–387.
12. Gold SI, Hasselgren G. Peripheral inflammatory root resorption. A review
of the literature with case reports. J Clin Periodontol 1992: 19: 523–534.
13. Trope M. Root resportion of dental and traumatic origin: classification based
on Etiology. Pract Periodont Aesthet Dent 1998: 10: 515–522.
14. Levin L, Trope M. In: Hargreaves KM, Goodis HE, eds. Seltzer and Bender’s
Dental Pulp, revised edition. Quintessence Publishing Co, Inc, Chicago, London,
2002: 425–447.
15. Fuss Z, Tsesis I, Lin S. Root resorption – diagnosis, classification and
treatment choices based on stimulation factors. Dent Traumatol 2003: 19: 175–182.
16. Tronstad L. Root resorption – etiology, terminology and clinical manifestations.
Endod Dent Traumatol 1988: 4: 241–252.
17. Harrington GW, Natkin E. External resorption associated with the bleaching
of pulpless teeth. J Endod 1979: 5: 344–348.
18. Heithersay GS, Dahlstrom SW, Marin PD. Incidence of invasive cervical resorption
in bleached root-filled teeth. Aust Dent J 1994: 39: 82–87.
19. Trope M, Chivian N, Sigurdsson A, Vann WF Jr. In: Cohen S, Burns RC, eds.
Pathways of the Pulp, 8th edn. St Louis: Mosby, 2002: 626–628.
20. Heithersay GS. Invasive cervical resorption: an analysis of potential predisposing
factors. Quintessence Int 1999: 30: 83–95.
21. Wedenberg C, Lindskog S. Evidence for a resorption inhibitor in dentin. Scand
J Dent Res 1987: 95: 270–271.
22. Heithersay GS. Clinical endodontic and surgical management of tooth and associated
bone resorption. Int Endod J 1985: 18: 72–79.
23. Heithersay GS. Treatment of invasive cervical resorption: an analysis of
results using topical application of trichloracetic acid, curettage, and resorption.
Quintessence Int 1999: 30: 96–110.
24. Pierce A, Lindskog S. The effect of an antibiotic/corticosteriod paste on
inflammatory root resorption in vivo. Oral Surg Oral Med Oral Pathol 1987: 64:
216–220.
25. Pierce A, Heithersay GS, Lindskog S. Evidence for direct inhibition of dentinoclasts
by a cortico-steroid/antibiotic endodontic paste. Endod Dent Traumatol 1988:
4: 44–45.
26. Bryson EC, Levin L, Branchs F, Abbott PV, Trope M. Effect of immediate intra-canal
placement of Ledermix Pasteson healing of replanted dog teeth after extended
dry times. Dent Traumatol 2002: 18: 316–321.
27. Heithersay GS. Combined endodontic–orthodontic treatment of transverse root
fracture in the region of the alveolar crest. Oral Surg Oral Med Oral Pathol
1973:
36: 414–415. 28. Ingber JS. Forced eruption. Part II. A method of treating non-restorable
teeth – periodontal and restorative considerations. J Periodontol 1976: 47: 203–216.
29. Heithersay GS. External root resorption. Ann R Aust Coll Dent Surg 1994:
12: 46–59. 30. Antrim DD, Altaras DE. Treatment of subosseous resorption: a case
report. J Endon 1982: 8: 18–23.
31. Pitt-Ford TR, Torabinejad M, McHendry DJ, Hong CU, Kariyawasam SP. Use of
mineral trioxide aggregrate for repair of furcal perforations. Oral Surg Oral
Med Oral Pathol 1995: 79: 756–763.
32. Koh ET, Torabinejad M, Pitt Ford TR, Brady K, McDonald F. Mineral trioxide
aggregrate stimulates a biological response in human osteoblasts. J Biomed Mater
Res 1997: 5: 432–439.
33. Frank A, Simon JHS, Abou-Rass M, Glick DH. Clinical and Surgical Endodontics.
Philadelphia: Lippincott, 1983: 147–154.
34. Lustman J, Ehrlich J. Deep external resorption: treatment by combined endodontic
and surgical approach. A report of 2 cases. Int Dent J 1974: 24: 203–206.
35. Goodman JR, Wolfe GN. The treatment of cervical external resorption in adolescents.
Br Dent J 1980: 149: 234–236.
36. Francischone CE, Costa CG, Francischone AC, Ribeiro HT, Silva RJ. Controlled
orthodontic extrusion to create gingival papillae: a case report. Quintessence
Int 2002: 33: 561–565.
37. Rankow HJ, Krasner PR. Endodontic applications of guided tissue regeneration
in endodontic surgery. J Endod 1996: 22: 34–43.
38. Trope M. Subattachment inflammatory root resorption: treatment strategies.
Pract Periodont Aesthet Dent 1998: 10: 1005–1010.
39. Lindskog S, Blomlof L. Quality of periodontal healing. 1V: enzyme histochemical
evidence for an osteoblast origin of reparative cementum. Swed Dent J 1994: 18:
181–189.
40. Vincentelli R, Lepp FH, Boyssou M. Les taches to sees de ca cou ronne (‘pink
spots’) – leurs localisation intra et extra camerales. Schweiz Monatsschr Zahnheilkd
1973: 88: 1132–1150.
41. Hammarstrom L, Lindskog S. Factors regulating and modifying dental root resorption.
Proc Finn Dent Soc 1992: 88(Suppl 1): 115–123.
42. Heithersay GS,Wilson DF. Tissue responses in the rat to trichloracetic acid
– an agent used in the treatment of invasive cervical resorption. Aust Dent J
1988: 33: 451– 461.
43. Lindskog S, Blomlof L, Hammarstrom L. Evidence for a role of odontogenic
epithelium in maintaining periodontal space. J Clin Periodontol 1988: 15: 371–
373.
44. Leedham MD. The relationship between the epithelial cell rests of Malassez
and experimental root resorption and repair in Macaca fascicularis. MDS Thesis,
University of Adelaide, 1990.
45. Brice GL, Sampson WJ, Sims MR. An ultrastructural evaluation of the relationship
between epithelial rests of Malassez and orthodontic root resorption and repair
in man. Aust Orthod J 1991: 12: 90–94.
46. Dreyer CW. Clast cell activity in a model of aseptic root resorption. PhD
Thesis, University of Adelaide, 2002.
47. PierceAM,Lindskog S,HammarstromL.Osteoclasts: structure and Function. Electron
Microsc Rev 1991: 4: 1–45.
48. Pierce AM. Experimental basis for the management of dental resorption. Endod
Dent Traumatol 1989: 5: 255– 265.
49. Boyle WJ, Simonet WS, Lacey DL. Osteoclast differentiation and activation.
Nature 2003: 423: 337–342.
50. Collins MT, Bianco P. Fibrous dysplasia. In: Primer on the Metabolic Bone
Diseases and Disorders of Mineral Metabolism, 5th edn.Washington, DC: American
Society for Bone and Mineral Research, 2003: 466–470.
51. Andreasen JO, Andreasen FM. Textbook and Color Atlas of Traumatic Injuries
to the Teeth, 3rd edn. Copenhagen: Munsksgaard, 1994: 366–370.
52. Schajowicz F. In: Histological Typing of Bone Tumours, 2nd edn. Berlin: Springer-Verlag,
1993: 36–42. 53. Andreasen JO, Andreasen FM. Textbook and Color Atlas of Traumatic
Injuries to the Teeth, 3rd edn. Copenhagen: Munskgaard, 1994: 370–372.
54. Wedenberg C. Development and morphology of internal resorption in teeth –
a study in humans, monkeys and rats. PhD Thesis, Karolinska Institute, Stockholm,
1987: 22–23.
55. Rabinowitch BZ. Internal Resorption: conference on the biology of the human
dental pulp. Oral Surg Oral Med Oral Pathol 1972: 33: 263–281.
56. Cvek M. Endodontic management of traumatised teeth. In: Andreasen JO, Andreasen
FM, eds. Textbook and Color Atlas of Traumatic Injuries to the Teeth, 3rd edn.
Copenhagen: Munskgaard, 1994: 560–561.
57. Velasques-Plata D, Scheyer ET, Mellonig JT. Clinical comparison of an enamel
matrix derivative used alone or in combination with a bovine-derived xenograft
for the treatment of periodontal osseous defects in humans. J Periodontol 2002:
73: 433–440.
58. Sculean A,Windisch P, Keglevich T, Chiantella GC, Gera I, Donos N. Clinical
and histologic evaluation of human infrabony defects treated with an enamel matrix
protein derivative combined with a bovine-derived xenograft. Int J Periodontics
Restorative Dent 2003: 23: 47–55.
59. Lyon KF. Subgingival odontoclastic resorptive lesions: classification, treatment
and results in 58 cases. Vet Clin North Am Small Anim Pract 1992: 22: 1471–1483.
60. Harvey CE. Feline dental resorptive lesions. Seminars Vet Med Surg (small
animals) 1993: 8: 187–196.
[powrót] |